Introduction
The term “body image” has generally been defined as the mental representation that one has of his/her body or physical appearance and encompasses two components: perceptual and attitudinal 1, 2, 3.
A particular issue that has perceived a lot of attention is body image distortion (BID). BID may result in an erroneous perception of body image and, in addition, a negative feeling about the body 4 and it can occur in two directions: overestimation (people believe themselves to be fatter than they really are) and underestimation (people believe that they are thinner than they really are) 5, 6. Perception of body size is one mechanism of weight regulation and it is indispensable in maintaining an appropriate weight. When BID appears, this mechanism is altered and may be unhealthy regardless if the direction of the distortion is by overestimation or underestimation. On the one hand, underweight or normal weight people who overestimated their body size feel fat, and in order to achieve an almost impossible thin ideal body image may develop unhealthy-related behaviors such as excessive exercise, disordered eating, smoking, as well negative psychological consequences such as poor self-esteem and depression 7. On the other hand, overweight and obese people who underestimated their body size are not conscious that they must lost weight to avoid health risks such as coronary heart disease, type 2 diabetes mellitus, high blood pressure, strokes, high cholesterol or sleep apnea 8.
An important reason for the appearance of BID is social pressure from the media 9, 10. In Western cultures, thinness is rewarded and fatness is punished 11, 12. Overweight and obese people are far from the typical aesthetic standards and, for this reason, they are discriminated against by society 13. They are considered lazy and incompetent and have a lot of problems in some areas such as employment or social relationships 14. However, not all obese people are equally vulnerable to this problem and, furthermore, BID is not limited uniquely to overweight and obese people but may also affect underweight and normal weight people 15, 16. This is because BID cannot only be attributed to social pressure but involves a complex web of perceptual, emotional, psychological and behavioral factors 17.
For all these reasons, the evaluation of BID is considered crucial to better understanding the problems which stem from over and underestimation and to develop better and more efficient intervention programs.
This evaluation may be carried out by means new technologies. In the literature, there are reports that have studied BID using the conventional administration modes such as paper and pencil but few of them have used online questionnaires for this purpose. The advantages of online questionnaires over traditional administration methods are numerous. The online questionnaires allow collecting data continuously, regardless of day or time. Moreover, these questionnaires are less expensive and can be conducted in large samples. Another advantage is the speed and precision of data collection because responses from online questionnaires can be mechanically stored on databases or statistical packages18,19,20 .
In light of these considerations, this study assesses BID in young university students employed an online visual scale to measure 1) gender differences 2) their influence in self-esteem and negative eating attitudes of body image distortion 3) the predictive ability of self-esteem and negative eating disorders for body image distortion.
Material and methods
Participants
This study was carried out using a transversal design. A convenience sampling was selected because of the limitations of time, money and staff. A total of 459 university students at Universitat Politècnica de València consisting of 203 women and 256 men with an average age of 21.34 years (SD = 3.49) participated in this study. Their respective body mass index (BMI) were 21.42(SD = 2.76)) and 23.50 (SD = 2.71)) calculated from self-reported height and weight.
Measures and instruments
An online visual scale of figures was used to measure the perceived body mass index (PBMI). PBMI was compared to the body mass index (BMI) to measure the accuracy of body size estimation 6.
The online visual scale of figures includes a series of nine frontal male figures (for male responses) and a series of nine frontal female figures (for female responses) 21. These figures progressively increase their body size ranging from very thin (1) to very fat (9). Participants were asked to indicate which figure from the online visual scale they thought better represented to their current body image and, after, these figures were included into one of the following four groups: underweight (figures 1, 2 and 3), normal weight (figures 4 and 5), overweight (figures 6 and 7) and obese (figures 8 and 9)22.
The BMI, calculated by means of self-reported weight and height, was classified into the same four groups used to classify the PBMI: underweight (BMI < 19.99 kg/m2), normal weight (20.00 kg/m2 < BMI < 24.99 kg/m2), overweight (25.00 kg/m2 < BMI < 29.99 kg/m2) and obese (BMI > 30.00 kg/m2).
BID scores were calculated for each participant as the resulting from the difference between PBMI and BMI. A result equal to 0 signified no distortion. The results different from 0 signified misperception and were classified according to the direction and the degree. According to the direction, participants were classified into two categories: “lower” (the result of the discrepancy was negative) and “higher” (the result was positive). Participants classified as “lower” meant that they underestimated their body size because they believed they were thinner than they really were whereas participants classified as “higher” signified that they overestimated their body size because they believed they were fatter than they really were. According to the degree of misclassification, participants were also classified into two categories: mild misperception (the result of the difference was equal to 1, in other words, PBMI was close to the BMI) and gross misperception (the result of the difference was greater than or equal to 2 or the PBMI was far from the BMI).
Rosenberg’s Self-Esteem Inventory (RSES) 23,24 and Eating Attitudes Test-26 (EAT-26)25,26 were adapted to be used in an online way.
RSES is a 10 item measure used for the evaluation of global self-esteem and scores range from 10 (low self-esteem) to 40 (large self-esteem).
EAT-26 was the tool used to measure negative eating attitudes. The online tool is composed of 26 items and scores range between 0 and 78. Higher scores mean higher negative eating attitudes.
Procedure
The study was approved by the Human Research Ethical Committee at the University of Universitat Politècnica de València. Data collection took place in the university library where were found students from different faculties, different genders and a wide age range. There were two inclusion criteria: being enrolled in UPV during the academic year and being 30 years old or less. Participants completed a battery of online self-reported questionnaires in a classroom with computers without time limit. Researchers were present to answer any possible questions. The questionnaires were anonymous and confidential. All participants took part on a voluntary basis and were considered to imply informed consent.
Statistical analysis
Descriptive statistics across gender were calculated using frequencies, percentages and chi-square tests on categorical variables, and the mean (M) and standard deviation (SD) on continuous data. The accuracy of body size estimation was calculated by means of Cohen´s kappa using the BMI as a criterion and examining the proportion of subjects that fell into the same group, into the closest groups, and into the farthest groups according to the PBMI. A series of one-way ANOVAs was conducted between categories of BID (dependent variable), self-esteem and negative eating attitude scores (independent variables) in order to determine if there were any significant differences in self-esteem and negative eating attitudes according to BID. Tukey post-hoc tests were used to test group differences when assumptions of homogeneity of variance were found and Games-Howell when they were not. Pearson correlation coefficients were calculated to assess the degree of association between BID, self-esteem and negative eating attitudes. Multiple linear regression analysis was conducted to determine whether self-esteem and negative eating attitudes scores could predict BID. The statistical Program for Social Sciences (SPSS) version 16.5 and a statistical significance level of .05 was used in all analyses.
Results
Body mass index and perceived body mass index
Table 1 shows the classification of the participants into underweight, normal weight, overweight and obese according to the BMI and the PBMI. The BMI, calculated from self-reported weight and height, indicated that approximately two thirds of the whole sample was classified as normal weight, mostly represented by men. Only 17.9 % of the participants fell within the underweight category, overrepresented by women. Just 15.7% and 2.0% of the whole sample were overweight and obese, respectively, mostly being men. A significant gender effect on the BMI was observed (χ(3)² = 57.979, p < .001).
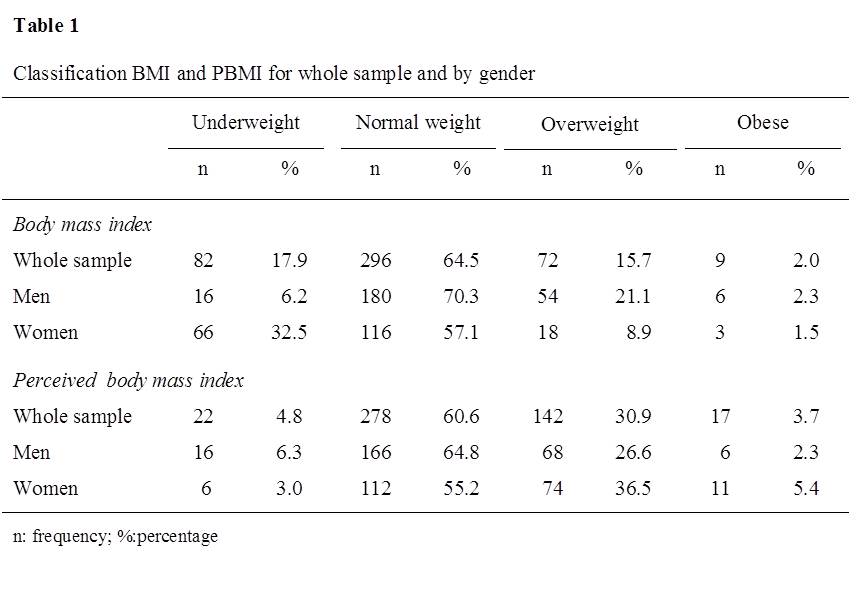
The PBMI, calculated from the figure selected as current body size, suggested that about two-in-three of the participants considered themselves to be normal weight, of these the percentage of men was higher than women. A sizable proportion of participants perceived that they were overweight, mostly women. Fewer participants saw themselves as obese or underweight. The obese group was mostly represented by women whereas the underweight group by men. A significant gender effect on the PBMI was observed (χ(3)² = 10.783, p < .05).
Body image distortion
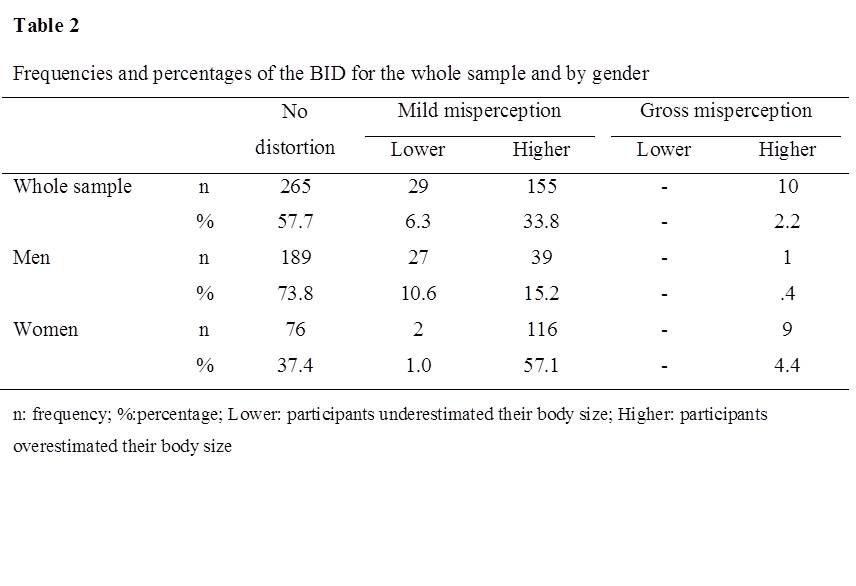
Table 2 shows the frequencies and the percentages of BID for the whole sample and by gender. Approximately half of the whole sample reported distortion. Of those, only 6.3% underestimated their body size, whereas 36.0% indicated overestimation. Mild misperception was more prevalent than gross misperception (40.1% vs. 2.2%).
Gender differences in BID found that the percentage of women that did not have a realistic perception of their body size was higher than the percentage of men (62.6% v. 26.2%). According to the direction, men were more likely to underestimate their body size than women (10.6% vs. 1.0%) whereas overestimation was more prevalent in women (61.5% vs. 15.6%). According to the degree of misperception, gross misperception was represented mostly by women (4.4% vs. 0.4%) but only in the direction of overestimation.
Agreement between BMI and PBMI
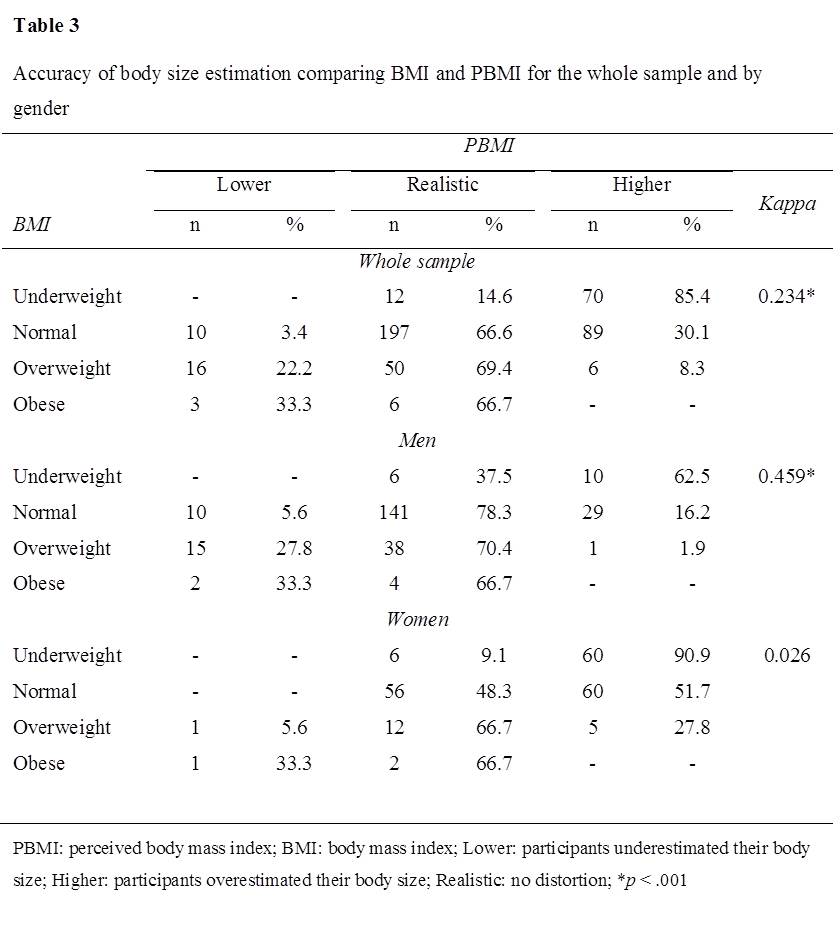
Table 3 displays the percentage of participants classified in BMI categories to the percentages classified in perceived categories. Participants classified as normal weight, overweight and obesity according to their BMI had a more realistic appreciation of their body size than those classified as underweight. Underweight participants mostly perceived themselves as “higher”, overrepresented by women. In contrast, a sizable percentage of overweight and obese participants saw themselves as “lower”.
Cohen´s kappa was used to measure the agreement of participants in each BMI with their PBMI. For the whole sample, Cohen´s kappa suggested a weak agreement. By gender, a moderate agreement was obtained for men but no agreement for women.
Self-esteem and negative eating attitudes according to BID
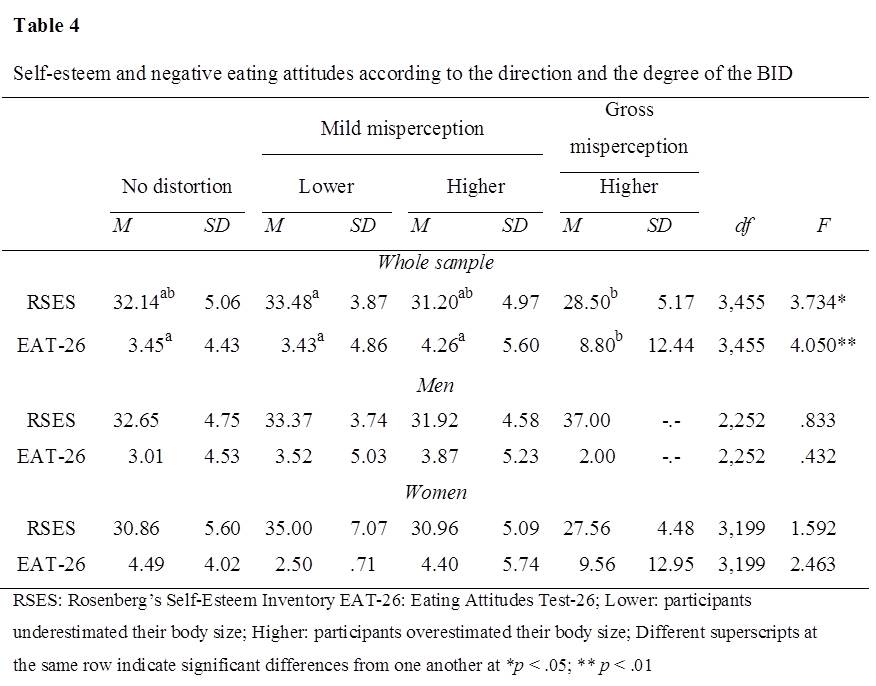
Table 4 displays a series of one-way ANOVA conducted to examine if there were any significant differences in self-esteem and negative eating attitude scores according to BID. For the whole sample, according to the degree of misperception, gross misperception supposed lower self-esteem and higher negative eating attitude scores than mild misperception. According to the direction, participants who underestimated their body size were the most likely to exhibit higher self-esteem and lower negative eating attitudes scores. It is important to note, that surprisingly, participants without distortion obtained lower self-esteem and higher negative eating attitude scores than those who underestimated their body size. Post-hoc test revealed differences in self-esteem scores between participants who underestimated their body size and those who grossly overestimated it, whereas in negative eating attitudes the differences were between participants who grossly misperceived their body size and the other groups. Considering genders, results indicated no significant differences in self-esteem and negative eating attitudes according to the BID in either gender.
Pearson correlation coefficients were calculated between BID and self-esteem and negative eating attitudes for whole sample and for both genders separately. For the whole sample, BID was significantly negatively related to self-esteem (r = - 0.093, p <.05) and significantly positively associated with negative eating attitudes (r = 0.121, p <.05), suggesting that the greater the BID, the lower the self-esteem and the higher the negative eating disorders. When the correlations were studied by gender, no significant associations were found in either gender.
Multiple regression indicated that negative eating attitudes was a weak predictor (β = .010; t =1.993; p < .05) explaining only 5.9% of the variance of BID and self-esteem did not effectively predict body image distortion. By genders, neither negative eating attitudes nor self-esteem were predictors of BID.
Discussion
This paper discusses BID in university students in relation to gender, self-esteem and negative eating attitudes using an online visual scale. The results suggested that almost half of the whole sample reported distortion. This report found remarkable gender differences in prevalence, direction and degree of distortion.
Regarding prevalence of the distortion, men in this study were more likely to report realistic perceptions of their body size, whereas women were more prone to express distortion. In addition, Cohen´s k corroborated that men were more accurate in their body size estimation than women.
According to the direction of the BID, the results of this report were in line with the generous body of evidence that used a paper-pencil visual scale. Women are more likely to feel too fat, wishing to be smaller, whereas a feeling of being too thin, wishing to be bigger, is more established in males 27, 28, 29, 30. Two possible reasons might explain the overestimation reported in women and underestimation in men. The first explanation is based on the differences in women and men´s ideal body image, thinness for females and a lean and muscular physique for males 31, 32. The second explanation is derived from the mistake made by both men and women in their assessment of what the opposite sex would find most attractive. A number of studies have found that women presume that men find a thinner body more attractive than men actually report liking, whereas men perceive that women desire more muscularity than women express liking 33, 34, 35, 36.
Regarding the degree of the BID, the result of this report indicated that higher levels of misperception were more prevalent in women, whereas men perceived their body image closer to their BMI 37. This result may be explained by the fact that women receive more social pressure such as images, advertisements or messages about the need to be increasingly thin to be closer to an almost unattainable ideal body image. Furthermore, men give more importance to the opposite sex´s body image than women do, adding more pressure to women.
The accuracy of body size estimation was measured by means of comparing BMI and PBMI. It was found that underweight participants tended to overestimate their size, whereas obese participants were more likely to underestimate it. The association between BMI and body image is rather complex and there are two opposing findings. One the one hand and in the line of the result obtained in this report, some studies have expressed that obese people underestimate their size to a higher level than those classified as normal weight 38. On the other hand, other studies conclude that obese people are more likely to report overestimation 39.
When examining the results of the correlation coefficients by gender, there was no association between BID and self-esteem. Previous research findings in this area have been divergent, some findings only indicate association between BID and self-esteem for women and others failed to find significant association for either gender. Some of the postulated reasons for the inconsistent findings could include methodological differences in measuring self-esteem and BID or differences in the sociodemographic factors of the sample.
Limitations
The limitations of this report must be acknowledged. Firstly, in this study BMI corresponded to the BMI calculated from self-reported weight and height. The problem is that self-reported weight tends to be underestimated whereas self-reported height is often overestimated, leading to underestimation of BMI. The use of self-reported measures is justifiable in this study if it is taken account that self-reported height and weight measures have been used in a large number of surveys 40, 41 and furthermore, the values of self-BMI obtained in this report were moderately consistent with those obtained by means of objective measures for Spain university students with a similar age range 42. The second limitation was related to the conclusions because they must be limited to a university environment. For other environments, the conclusions should be interpreted carefully.
References
1. Alsaker FD. Pubertal timing. Overweight and psychological adjustment. J Early Adolescence. 1992;12:396–419.
2. Garner DM, Garfinkel PE. Body image in anorexia nervosa: Measurement, theory and clinical implications. Int J Psychiatry Med.1981;11:263–284.
3. Slade P. Body image in anorexia nervosa. Br J Psychiatry.1988;153:20–22.
4. Skrzypek S, Wehmeier PM, Remschmidt H. Body image assessment using body size estimation in recent studies on anorexia nervosa. A brief review. Eur Child Adolesc Psychiatry. 2001;10:215–221.
5. Liechty JM. Body image distortion and three types of weight loss behaviors among nonoverweight girls in the United States. J Adolesc Health, 2010:47:176–182.
6. Paap CE, Gardner RM. Body image distortion and relationship satisfaction among college students. Pers Individ Dif. 2011;51:715–719.
7. Annis NM, Cash TF, Hrabosky JI. Body image and psychosocial differences among stable average weight, currently overweight, and formerly overweight women: the role of stigmatizing experiences. Body Image, 2004;1:155–167.
8. Lucove JC, Huston SL, Evenson KR. Workers’ perceptions about worksite policies and environments and their association with leisure-time physical activity. American J Health Promot. 2007;21:196–200.
9. Heinberg LJ, Thompson JK. Body image and televised images of thinness and attractiveness: A controlled laboratory investigation. J Soc Clin Psychol, 1995;14:325-338.
10. Tiggemann M. The role of media exposure in adolescent girls’ body dissatisfaction and drive for thinness: Prospective results. J Soc Clin Psychol, 2006;25:523-541.
11. Dittmar H, Lloyd B, Dugan S, Halliwell E, Jacobs N, Cramer H. The ‘‘body beautiful’’: English adolescents’ images of ideal bodies. Sex Roles,2000;42: 887–915.
12. Nichter M, Nichter, M. Hype and weight. Medical Anthropology, 1991; 13: 249-284.
13. Puhl R, Brownell KD. Bias, discrimination, and obesity. Obes Res,2001;9:788–805.
14. Puhl R, Brownell KD. Confronting and coping with weight stigma: An investigation of overweight and obese adults. Obesity, 2006;14:1802–1815.
15. Abraczinskas M, Fisak Jr, Barnes RD. The relation between parental influence, body image, and eating behaviors in a nonclinical females sample. Body image, 2012;9:93-100.
16. Lawler M, Nixon E. Body dissatisfaction among adolescent boys and girls: The effects of body mass, peer appearance culture and internalization of appearance ideals. J Youth Adolesc, 2011;40:59-71.
17. Cash TF. Body image: past, present, and future. Body Image,2004;1:1–5.
18. Fleming CM, Bowden M. Web-based surveys as an alternative to traditional mail methods. J Environ Manag. 2009;90:284-92.
19. Thompson FE, Subar AF, Loria CM, Reedy JL, Baranowski T. Need for technological innovation in dietary assessment. J Am Diet Assoc. 2010; 110 (1): 48-51.
20. Vandelanotte C, Matthys C, De Bourdeaudhuij I. Reliability and validity of a computerized questionnaire to measure fat intake in Belgium. Nutr Res. 2004; 24: 621-31.
21. Stunkard A. Old and new scales for assessment of body image. Percept Mot Skills, 2000;90(3 Pt 1):930.
22. McElhone S, Kearney JM, Giachetti I, Zunft HF, Martinez JA. Body image perception in relation to recent weight changes and strategies for weight loss in a nationally representative sample in the European Union. Public Health Nutr, 1999;2:143–151.
23. Rosenberg M. Society and the adolescent self-image. Princeton: Princeton University Press. 1965.
24. Martín-Albo J, Núñez JL, Navarro JG, Grijalvo F. The Rosenberg Self-Esteem Scale: Translation and Validation in University Students. Span J Psychol, 2007;10:458–467.
25. Garner DM, Olmsted MP, Bohr Y, Garfinkel PE. The Eating Attitudes Test: Psychometric features and clinical correlates. Psychol Med, 1982;12:871-878.
26. Castro J, Toro J, Salamero M, Guimerá E. The eating attitudes test: Validation of the Spanish version. Evaluación Psicológica, 1991;7:175-190.
27. Bish CL, Blanck HM, Maynard LM, Serdula MK, Thompson NJ, Khan LK. Health-related quality of life and weight loss among overweight and obese U.S. adults, 2001 to 2002. Obesity (Silver Spring), 2006;14:2042–2053.
28. Gardner RM, Jappe LM, Gardner L. Development and validation of a new figural drawing scale for body-image assessment: The BIAS-BD. J. Clin. Psychol, 2009;65:113–122.
29. Leonhard ML, Barry NJ. Body image and obesity: effects of gender and weight on perceptual measures of body image. Addict Behav, 1998;23:31–34.
30. Raudenbush B, Zellner DA. Nobody’s satisfied: effects of abnormal eating behaviors and actual and perceived weight status on body image satisfaction in males and females. J Soc Clin Psychol, 1997;16:95–110.
31. Pope HG Jr, Olivardia R, Borowiecki JJ 3rd, Cohane GH. The growing commercial value of the male body: A longitudinal survey of advertising in women’s magazines. Psychother Psychosom, 2001;70:189–192.
32. Rohlinger DA. Eroticizing men: Cultural influences on advertising and male objectification. Sex Roles, 2002;46:61–74.
33. Cohn LD, Adler NE. Female and male perceptions of ideal body shapes: Distorted views among Caucasian college students. Psychology Of Women Q, 1992;16: 69-79.
34. Fallon AE, Rozin P. Sex differences in perceptions of desirable body shape. J. Abnorm. Psychol., 1985;94:102–105.
35. Huon GF, Morris SE, Brown LE. Difference between male and female preferences for female body size. Austral Psychol. 1990;25:314–317.
36. Rozin P, Fallon A. Body image, attitudes to weight, and misperceptions of figure preferences of the opposite sex: a comparison of men and women in two generations. J. Abnorm. Psychol, 1988;97:342–345.
37. Thompson JK, Thompson CM. Body size distortion and self-esteem in asymptomatic, normal weight males and females. Int J Eat Disord., 1986;5:1061–1068.
38. Tehard B, Van Liere MJ, Nougué C, Clavel-Chapelon F. Antropometric measurements and body silhouette of women: Validity and perception. J Am Diet Assoc, 2002;102:1779-1784.
39. Lemon SC, Rosal MC, Zapka J, Borg A, Andersen V. Contributions of weight perceptions to weight loss attempts: Differences by body mass index and gender. Body Image, 2009;6:90–96.
40. Fonseca, H., & de Matos, F. M. Perception of overweight and obesity among Portuguese adolescents: an overview of associated factors. Eur J Public Health, 2005;15:323–328.
41. Sánchez-Villegas A, Madrigal H, Martínez-González MA, Kearney J, Gibney M, de Irala J, et al. Perception of body image as indicator of weight status in the European Union. J Hum Nutr Diet, 2001;14:93-102.
42. Muñoz-Cachón MJ, Salces I, Arroyo M, Ansotegui L, Rocandio AM, Rebato E. Overweight and Obesity: Prediction by Silhouettes in Young Adults. Obesity, 2008;17:545–549.